About sub-acromial shoulder pain (SASP)
What is SASP?
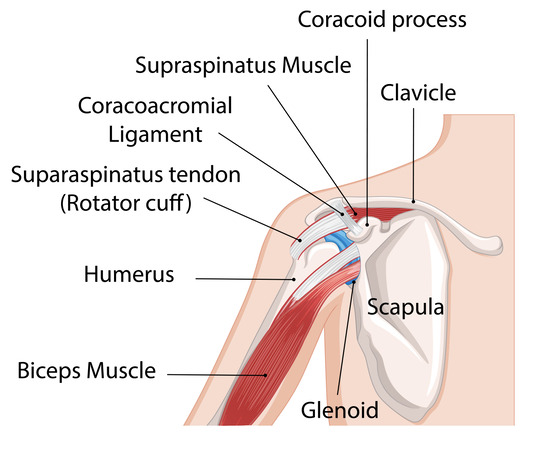
- SASP is the medical name for pain arising from the sub-acromial space of the shoulder.
- It is also commonly referred to as shoulder impingement or rotator cuff related shoulder pain.
- There are a number of structures in the sub-acromial space that can cause pain – these include the sub-acromial bursa and rotator cuff tendons
- SASP incorporates all conditions related to these structures that could cause pain – such as sub-acromial bursitis, rotator cuff degeneration or tendinopathy and rotator cuff tears.
- Pain is commonly located at the top and outside of the shoulder, aggravated by overhead activities and can cause night pain.
Watch the sub-acromial shoulder pain video (Credit to Somerset NHS Foundation Trust).
What causes SASP?
- The main cause is believed to be excessive load on the shoulder tissues, which can be over a long period of time or sudden.
- Repetitive movements at or above shoulder height and heavy lifting.
- Studies have shown links between SASP and metabolic syndromes such as diabetes, obesity, high cholesterol and high uric acid levels which can cause systemic inflammation.
Facts about sub-acromial shoulder pain(SASP)
- It affects 1 in 5 people at some stage in their life
- SASP is the most common disorder of the shoulder
- SASP is common in individuals who do heavy manual work
- Typically affects people between the ages of 35 and 75
- Accounts for between 44% to 65% of all shoulder complaints
Treatments and management
There are various treatment options available for SASP. These include education, pain management, exercise and potential surgery. In most cases imaging tests such as x-rays, magnetic resonance images (MRIs), or ultrasounds are not required to diagnose SASP. Scans are not always useful in diagnosing shoulder pain and although they can provide information about how the shoulder structures look, they don’t always change the treatment or management options available. Still, health care providers do sometimes arrange them to help diagnosis and to help guide treatment and management.
Patient education
Patient education is an important part of the management of SASP. Knowing more about the condition can help alleviate fears and concerns. Simple advice regarding modifying your daily activities can reduced the stress or load on your shoulder and help symptoms.
Pain management
- Paracetamol is a common painkiller which can be used to help treat your shoulder aches and pain. However, you should not take this with anything else that contains paracetamol.
- Anti-inflammatory medication (NSAIDs): These include medications such as Ibuprufen, Diclofenac, and Naproxen which can help ease pain and reduce any inflammation in the shoulder. These are usually only recommended in short course with advice from your GP or pharmacist.
- Steroid injection: Cortico-steroid is a powerful anti-inflammatory drug that can be injected into the sub-acromial space or bursa. It is important to know that this is not a cure, however it can give good pain relief to allow symptoms to be more manageable.
Continuing with physiotherapy and your exercise programme following steroid injections is important to achieve longer benefits and pain relief
Patient information
Exercise
Exercise
- Exercise is the main focus of treatment for SASP with the aim to help improve pain, restore shoulder movement and improve strength and overall function.
- It helps release chemicals called endorphins which reduce your perception of pain and trigger positive feelings.
- Exercise also improves blood flow to the affected area and can prevent the shoulder getting weak.
- Your physiotherapist will advise you on the appropriate exercises which generally include postural, stretches and strengthening exercises as a home exercise program.
- It can take 6 to 12 weeks to start to notice improvement in symptoms.
- Your physiotherapist may also try some mobilization techniques alongside your exercises.
Please note: Image generated using AI.
Other lifestyle changes
Other lifestyle changes
We know that physical inactivity and a sedentary lifestyle increases the likelihood of developing musculoskeletal pain along with other health problems such as type ii diabetes, stroke and cancer. Physical activity can help reduce the risk of all of the above mentioned conditions.
Smoking has an effect on every tissue in the human body, including muscle, bone and tendons and also slows and delays the healing process. Smokers are more likely to develop musculoskeletal pain including SASP compared to non-smokers. Stopping smoking can help your recover and speed up your recovery.
Surgical treatment
Surgical treatment
Patients with SASP rarely require surgery and it is only considered as a last resort if symptoms persist and are severe in spite of appropriate non-surgical treatment for at least 6 months.
Surgery generally involves shaving some of the bone away from under the roof of the shoulder (the acromion) and (or) repairing the torn tendons if required. You may need a prolonged period of Physiotherapy and activity modification after surgery.
Research suggests that surgery is not guaranteed to improve your shoulder pain, function and quality of life and that a large proportion of the benefits gained from surgery are related to the post-surgical recovery and rehabilitation.
Should referral for surgery be required then your clinician will discuss this with you further. As with all types of surgery there is a potential risk of post-operative complications.