About shoulder instability
What is shoulder instability?
Shoulder instability means the shoulder can dislocate (fully slip out of the socket) or subluxate (partially slip out of the socket) repeatedly during active movement or exercise. Subluxate means the joint moves more than it should do in normal circumstances but doesn’t actually come out of joint. There can be a number of reasons for this and this will determine the type of treatment you will receive.
Shoulder instability is divided into three main categories (this is largely dependent on the first episode of dislocation
Traumatic dislocation
This is where the shoulder undergoes an injury with enough force to pull the shoulder out of joint such as being tackled in a football or rugby game or a road traffic accident. It is much more common in men under the age of 30.
Usually the shoulder requires putting back in at an A&E department. Following a first time dislocation, the arm is usually put in a sling for a period of time and in some cases you may undergo a course of physiotherapy.
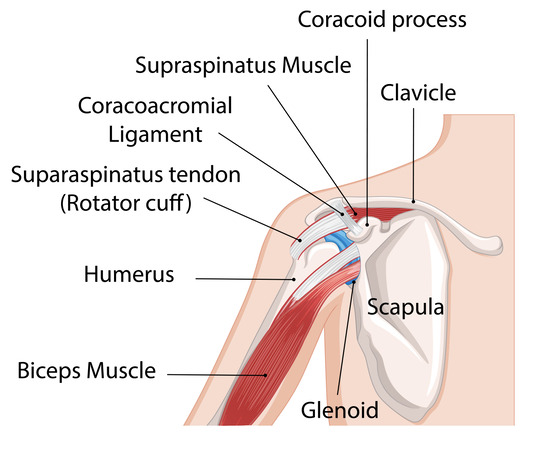
The shoulder joint is a ball and socket joint, which is held together by a combination of ligaments and muscles. There is also a rim of cartilage around the socket. If the rim of cartilage is damaged the shoulder can remain unstable with risk of further dislocation. Shoulder stabilisation surgery is an operation to repair the damage to the rim of cartilage and therefore re-stabilise the shoulder joint.
Non-traumatic instability
This occurs when the shoulder dislocates with minimal force such as reaching up for an object or turning over in bed. Repeated shoulder movements may gradually stretch out the soft tissue capsule around the joint. This can happen with athletes such as throwers and swimmers. Some people have naturally lax shoulder joints (hyper-mobility) which are more likely for the joint to slip out of place.
This can produce an imbalance in the control of the joint. Usually it will ‘pop’ back in itself or with a little help. Normally this type of dislocation does not need reducing in A&E. Referral for appropriate physiotherapy is the initial form of management.
Positional non-traumatic dislocations
This group of people can dislocate their shoulders without any form or history of trauma. This type of dislocation is usually painless and can be put back in easily. Both shoulders are typically involved.
The cause of this type of dislocation is usually a result of what we call ‘abnormal muscle patterning’ which means the strong muscles around the shoulder joint are not working in the correct order causing them to pull the shoulder out of joint with movement in the particular direction such as lifting the arm forward above the head or out to the side and above the head.
How is it treated?
Traumatic dislocation
Following a first-time dislocation, your arm may be put in a sling. Your doctor or physiotherapist will advise you on when to remove it and start exercise. Painkillers such as paracetamol can be used to dull the pain following shoulder dislocation. Anti-inflammatory tablets can also be effective. It is best to consult your GP or pharmacist before taking these medicines.
Non-traumatic instability
Physiotherapy is the initial form of management. The physiotherapist should look at the way in which the muscles and shoulder joint is moving and posture aiming to restore the balance. This is to provide stability to the shoulder joint. Treatment can ‘cure’ the problem as long as the exercises and advice is continued, but in some cases there may be minimal or nil benefit. At this point surgical intervention is indicated. (shoulder doc).
Positional non-traumatic dislocations
The main treatment for this is physiotherapy that looks at re-sequencing the muscles in order to prevent further dislocations. Occasionally surgery in the form of thermal capsular shrinkage or plication may be necessary.
Prevention
Strong shoulder muscles remain the best defence against shoulder dislocation, subluxation, and, thus, instability. Exercises that build up these muscles around the shoulder should be done. The key is to balance the muscles around the shoulder and ensure not only the ‘mirror’ muscles are exercises (those that you can see when looking in the mirror). Good core stability and posture are also important.
Adequate warm-up before activity and avoidance of high-contact sports will help prevent instability-causing injuries.