About hip impingement
What is hip impingement?
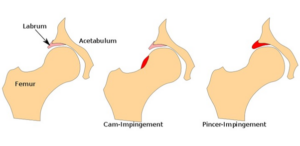
The hip joint is a ball and socket joint between the Femur (thigh bone) and the acetabulum (the hip socket). Hip impingement is caused by contact between the head due to bony changes on the ball or the socket. Repeated contact between the two bony surfaces can damage the hip labrum (cartilaginous structure surrounding the hip) which attaches to the rim of the hip socket, and can cause pain in the area. If this continues, it can lead to damage to the cartilage and eventually lead to osteoarthritis of the hip. There are 3 types of impingement depending on where the excess bone is:
- cam, excess on the ball
- pincer, excess on the socket
- mixed, excess on both bony elements
What causes hip impingement?
- Typically affects younger people who play lots of sport
- Genetics
- Excessive rotational sporting activity during adolescence, for example, football and rugby
- Obesity
- Decreased muscular strength and coordination around the hip
How can I tell if I have hip impingement?
- You may feel pain in the groin, down the front of the thigh, occasionally the outside of the hip and rarely the buttock region
- Running, changing direction, twisting or explosive movements will often reproduce pain
- You may get pain when you bring your knee towards your chest or perform a deep squatting movement, for example, tying shoe laces
- You may feel catching in the hip as you move or it may give way or feel like it may give way
How can hip impingement be treated?
Weight management
There is a link between impingement and obesity. Studies show a weight loss of 10% can provide a 50% reduction in symptoms, to calculate your target weight loss figure, multiply your body weight by 0.10. Excess body fat is also known to amplify inflammation around the body and so can cause increase in pain, losing weight can help avoid this. * Link to general health weight loss page *
Strength exercises
Improving movement control around the hip, core stability and overall strength of the hip muscles will help to improve the way your hip moves which can take the pressure off of the painful region. The exercises will begin in positions that are more comfortable and gradually progress to more difficult positions. The exercises need to be just right with regards to how much you do; too little will not be enough to increase your strength, too much will increase your pain. See the exercise plan for exercises and how to build these up.
General exercise
Moderate intensity exercise for examples fast walks, cycling, pilates or yoga class also help to strengthen the hip muscles and maintain your fitness levels. You may need to modify these to avoid reproducing the pain for example doing a class but skipping particularly painful exercises or doing them but with less depth and range. Exercise releases endorphins in the brain, the body’s natural painkiller, so can help with pain.
Activity modification
As with your exercises; too much activity can irritate symptoms and too little can lead to deconditioning. Feeling pain in the hip does not mean you are damaging the tissues, most pain that occurs after activity (without incident or trauma) is related to sensitivity of the muscles rather than damage. Try to take regular breaks and pace activities to avoid building up the sensitivity. Also try to avoid high impact exercise such as heavy squats or deadlifts or fast paced running on hard ground, these aren’t necessarily damaging but need to be carefully introduced, your physio will help you do this.
Optimise painkillers
You may be advised by your GP to take anti-inflammatory drugs which can help with pain and stiffness, as well as simple pain killers such as Paracetamol. Please see the NHS website for further information:
- Paracetamol for adults: painkiller for pain and high temperature, NHS
- Ibuprofen for adults: painkiller which also treats inflammation, NHS
Surgery
If the exercises and lifestyle changes do not help, then surgery may be an option. However, recent research has shown surgery to only be slightly more effective than physiotherapy in the management of this condition, after a year surgical patients were 60% better and physiotherapy patients were 50% better. We therefore we advise a good period of rehabilitation before potentially considering surgery, since operations carry more risk than doing rehabilitation exercises.